The Supplement Loading Phase: What It Is, When You Need One, and How to Get the Dose Right
Learn what a supplement loading phase is, which vitamins and supplements use one, how to determine the right dose, and when it's worth it.

Your doctor hands you a supplement protocol and says, “Take this higher dose for the first eight weeks, then drop down to maintenance.” You nod, but later you’re staring at the bottle thinking — why can’t I just take the normal dose from the start?
That higher-dose kickoff period has a name: the supplement loading phase. It’s one of the most common — and most misunderstood — parts of a supplement regimen. Some supplements genuinely need it, others don’t, and getting the dose wrong in either direction can slow your recovery or cause unnecessary side effects.
This guide breaks down exactly what a loading phase is, which supplements actually use one, how loading doses are determined, and how to stay on track when your protocol changes mid-stream.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult your healthcare provider before starting or changing any supplement regimen. The dosages referenced below are drawn from published clinical guidelines and are not personal recommendations.
What Is a Supplement Loading Phase?
A loading phase is a short period at the beginning of a supplement regimen where you take a higher-than-normal dose to rapidly build up your body’s stores of a nutrient. Once levels reach a target range, you transition to a lower maintenance dose to keep them there.
Think of it like filling a swimming pool. If the pool is nearly empty (a significant deficiency), a garden hose (maintenance dose) will work — eventually. But it’ll take months. A fire hose (loading dose) fills it up much faster. Once it’s full, you only need the garden hose to top it off and replace what evaporates.
The key distinction:
- Loading dose — higher amount, shorter duration, designed to saturate stores quickly
- Maintenance dose — lower amount, long-term, designed to sustain adequate levels
It’s important to distinguish a true loading phase from a simple build-up period. Some supplements — like omega-3 fatty acids — take weeks to reach steady-state levels in your body, but you take the same dose throughout. That’s not loading; that’s just how the nutrient works. A genuine loading phase means you deliberately take a higher dose first, then step down.
Not every supplement needs a loading phase. It depends on the nutrient, how depleted you are, and how your body stores and processes it.
Which Supplements Have Established Loading Protocols?
Loading phases are most established for a small group of supplements backed by clinical guidelines. Here’s a quick reference:
| Supplement | Typical Loading Dose | Loading Duration | Maintenance Dose | Source |
|---|---|---|---|---|
| Vitamin D | 50,000 IU/week | 6–12 weeks | 1,000–2,000 IU/day | Endocrine Society |
| Creatine | 20g/day (4 × 5g) | 5–7 days | 3–5g/day | ISSN Position Stand |
| Iron | 100–200mg elemental/day | 4–12 weeks | 30–65mg/day or alternate-day | ASH 2024 Guidelines |
| Vitamin B12 | 1,000 mcg/day IM | 7–14 days, then weekly × 4 | 1,000 mcg/month | Standard of care |
You’ll notice omega-3 is not on this list. While omega-3 fatty acids take 4–6 weeks to incorporate into cell membranes, the dose doesn’t change — you take 2–4g/day continuously for conditions like hypertriglyceridemia. That’s a therapeutic dose, not a load-then-reduce protocol. Including it as a “loading phase” supplement would be misleading.
Now let’s look at each one in more detail.
Vitamin D — The Most Common Loading Phase
If your blood levels of 25-hydroxyvitamin D are below 20 ng/mL, you’re clinically deficient. The Endocrine Society’s widely used protocol recommends 50,000 IU once a week for six to eight weeks, followed by a maintenance dose of 1,500–2,000 IU/day. For severe deficiency (below 10 ng/mL), some clinicians extend loading to 8–12 weeks or use 50,000 IU twice weekly for the first 2–3 weeks before stepping down to once weekly.
A few important details:
- The official upper tolerable intake level (UL) for vitamin D is 4,000 IU/day for adults (Institute of Medicine). A loading dose of 50,000 IU/week works out to about 7,100 IU/day — this is considered safe short-term under medical supervision, as the Endocrine Society notes that up to 10,000 IU/day is likely safe for adults without risk factors.
- Large single bolus doses (300,000+ IU) are falling out of favor. Research — including the Sanders et al. (2010) trial — showed that a single annual mega-dose of 500,000 IU actually increased fall and fracture risk, likely because the body rapidly inactivates the surge. Current consensus favors daily or weekly dosing over massive one-time boluses.
- Vitamin D toxicity occurs at serum levels above 150 ng/mL and manifests as hypercalcemia — nausea, vomiting, confusion, kidney stones, and in severe cases cardiac arrhythmias. This is rare at standard loading doses but is the reason monitoring matters.
- The half-life of 25(OH)D is approximately 2–3 weeks, which means the nutrient accumulates gradually — supporting weekly dosing schedules.
If you’re working through a vitamin D deficiency, you’re likely already on one of these protocols.
Creatine — The Classic Loading Phase
Creatine is the most well-known loading phase in the fitness world. The ISSN (International Society of Sports Nutrition) position stand recommends approximately 0.3g per kg of body weight per day for 5–7 days — roughly 20g/day for most adults, split into four 5g doses. After loading, you drop to 3–5g/day for maintenance.
Here’s what the evidence actually says:
- Loading saturates muscle creatine stores in about one week. Without loading, taking 3–5g/day reaches the same saturation in approximately 3–4 weeks (21–28 days). Both approaches work — loading just gets you there faster.
- The primary side effect is water retention of 1–2 kg (roughly 2–4 lbs) due to creatine’s osmotic effect in muscle cells. This is normal, harmless, and temporary.
- GI discomfort (bloating, cramping, diarrhea) can occur when large single doses are taken. Splitting into 4 × 5g doses and taking them with meals minimizes this.
- There is no credible evidence linking creatine to kidney damage, hair loss, or muscle cramps in healthy individuals at recommended doses (ISSN, 2017).
- A 2024 review in Nutrients reaffirmed these recommendations. Some researchers are exploring a middle-ground protocol — 10g/day for 10–14 days — to reduce GI issues while still reaching saturation faster than maintenance alone, though this isn’t a formal recommendation yet.
Who should be cautious: Individuals with pre-existing kidney disease should consult a physician before any creatine use. Those on medications affecting kidney function (certain NSAIDs, diuretics) should also check with their doctor.
Iron — Medically Supervised Loading
Iron loading is almost always done under medical supervision because excess iron is toxic — it can cause liver damage, heart problems, and oxidative tissue damage.
Traditional protocols call for 100–200mg of elemental iron per day (typically as ferrous sulfate 325mg tablets, each providing ~65mg elemental iron, taken 2–3 times daily) for 4–12 weeks. However, newer guidelines are shifting the approach:
- The 2024 ASH (American Society of Hematology) guidelines now emphasize alternate-day dosing — taking iron every other day rather than daily. Research by Stoffel et al. (Lancet Haematology, 2020) showed that alternate-day dosing of 40–80mg actually improves absorption efficiency due to hepcidin cycling. Your body upregulates hepcidin (a hormone that blocks iron absorption) after each dose, and giving it a day to reset means you absorb more from each tablet.
- IV iron (ferric carboxymaltose, iron sucrose) is recommended when: oral iron isn’t tolerated, absorption is impaired (celiac disease, IBD, post-bariatric surgery), rapid correction is needed, or hemoglobin is very low (below 8 g/dL with symptoms). IV formulations can fully replete stores in just 1–2 infusions.
- Treatment is generally indicated when ferritin is below 30 ng/mL and/or transferrin saturation is below 20%.
- After repletion, maintenance doses typically range from 30–65mg elemental iron per day or every other day.
- Monitoring should include ferritin and transferrin saturation every 3 months during loading, then every 6–12 months on maintenance. Ferritin above 300 ng/mL or transferrin saturation above 45% should prompt dose reduction.
Vitamin B12 — Injection vs. Oral Protocols
B12 loading protocols differ depending on severity and the underlying cause:
For pernicious anemia or severe deficiency (below 200 pg/mL):
- Injection protocol (standard): 1,000 mcg intramuscularly daily or every other day for 1–2 weeks (5–10 injections), then weekly for 4 weeks, then monthly indefinitely.
- High-dose oral alternative: 1,000–2,000 mcg/day orally. About 1% of oral B12 absorbs passively — bypassing the intrinsic factor pathway that’s impaired in pernicious anemia. While effective, injections remain the first-line approach for severe cases.
For dietary deficiency (vegetarians, vegans, elderly with poor absorption):
- Oral 1,000 mcg/day for 1–4 weeks, then 250–1,000 mcg/day as maintenance.
A note on forms: Cyanocobalamin has the most clinical trial data and is the standard in most repletion protocols. Methylcobalamin is bioactive and popular in consumer supplements, but has less robust evidence specifically for loading and repletion.
Why Not Just Start at the Maintenance Dose?
Fair question. For some supplements, you absolutely can — and should. But when a true deficiency exists, starting at maintenance has a real cost: time.
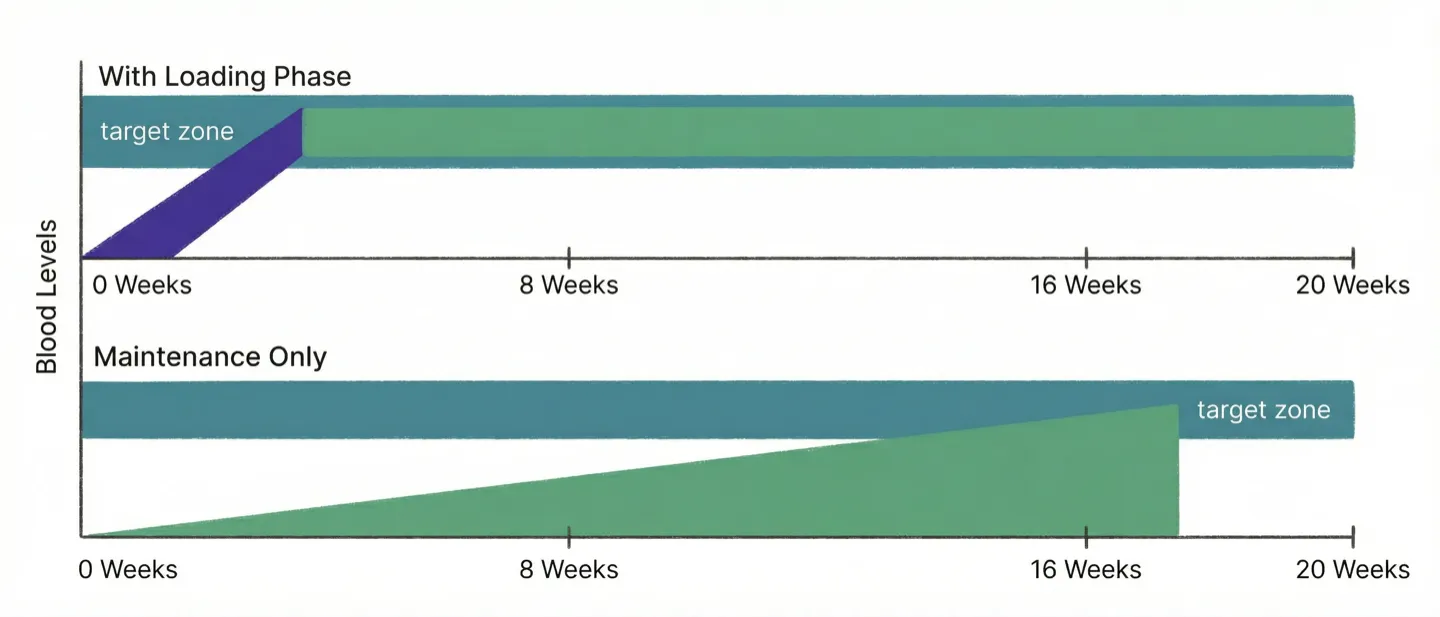
Consider vitamin D. Starting at a maintenance dose of 2,000 IU/day when your levels are severely low, it could take four to six months to reach an adequate range. With a loading protocol, you can get there in six to eight weeks — cutting recovery time roughly in half.
That time difference matters when you’re dealing with symptoms. Fatigue, bone pain, muscle weakness, mood changes — these don’t pause while you wait for your levels to rise.
For creatine, the calculus is simpler. Loading gets you peak performance benefits in one week instead of four. If you’re not in a rush, skipping the loading phase works just fine.
For iron-deficiency anemia, the stakes are higher. Severe anemia causes breathlessness, heart palpitations, and debilitating fatigue — symptoms that can meaningfully impact your ability to work and function. Faster repletion (especially via IV iron in severe cases) can make a significant quality-of-life difference.
The general rule: the more depleted you are, and the more your symptoms affect daily life, the more a loading phase makes sense.
How to Decide If You Need a Loading Phase
Not everyone needs one. Here’s a decision framework:
You likely need a loading phase if:
- Blood work shows a significant deficiency (not just borderline low)
- Your doctor or healthcare provider explicitly recommends one
- You’re experiencing symptoms tied to the deficiency that affect your daily life
- The supplement has an established clinical loading protocol (see the table above)
You probably don’t need a loading phase if:
- Your levels are borderline or mildly low (e.g., vitamin D of 20–29 ng/mL — considered “insufficient” but not deficient)
- You’re supplementing for general wellness or prevention, not treating a deficiency
- The supplement doesn’t have a recognized loading protocol — most water-soluble vitamins, magnesium, zinc, CoQ10, and omega-3s are taken at consistent doses
- You have kidney or liver concerns that make higher doses risky
The single most important factor is blood work. A loading phase without knowing your baseline levels is guessing — and with fat-soluble vitamins like D, guessing can lead to toxicity over time. Always test before you load.
How to Determine the Right Loading Dose
Loading doses aren’t one-size-fits-all. Your healthcare provider will consider several factors:
1. Severity of deficiency
The lower your levels, the more aggressive the loading protocol may need to be. Vitamin D protocols vary significantly by severity:
| Deficiency Level | 25(OH)D Range | Typical Approach |
|---|---|---|
| Severe | Below 10 ng/mL | 50,000 IU/week for 8–12 weeks; some start at twice weekly |
| Moderate | 10–20 ng/mL | 50,000 IU/week for 6–8 weeks |
| Mild (insufficiency) | 20–29 ng/mL | 1,000–2,000 IU/day; no formal loading needed |
2. Body weight and composition
Fat-soluble vitamins (D, A, E, K) are stored in adipose tissue. People with higher body fat may need larger loading doses to achieve the same blood levels. Some vitamin D protocols adjust the dose upward for individuals with a BMI over 30 — the Endocrine Society has noted that obese individuals may need 2–3 times the standard dose.
3. Absorption capacity
Certain conditions — Crohn’s disease, celiac disease, gastric bypass surgery, chronic pancreatitis — impair nutrient absorption. If your gut can’t absorb the standard oral dose efficiently, your provider may recommend a higher oral dose, alternate-day dosing (for iron), or switch to injections or IV infusions entirely.
4. Toxicity threshold and upper limits
Every nutrient has an upper tolerable intake level (UL). During loading, you may temporarily exceed the general UL under medical supervision — but there are hard limits:
- Vitamin D: UL of 4,000 IU/day (general), but up to 10,000 IU/day likely safe short-term. Toxicity risk above 150 ng/mL serum levels.
- Iron: No safe UL for supplemental iron — toxicity is dose-dependent and individual. Requires blood monitoring (ferritin, transferrin saturation).
- B12: No established UL — water-soluble with very low toxicity risk even at high doses.
- Creatine: No official UL, but doses above 20g/day are not recommended and offer no additional benefit.
5. Half-life of the nutrient
Nutrients with long half-lives accumulate more easily. Vitamin D’s half-life of about 2–3 weeks means weekly dosing works well — each dose builds on the previous one. Iron, on the other hand, triggers hepcidin production within hours, which is why alternate-day dosing can actually be more effective than daily dosing.
Bottom line: For anything beyond creatine, don’t self-prescribe a loading dose. Get blood work, work with a provider, and follow their protocol.
Common Myths About Loading Phases
Let’s clear up some misconceptions that circulate online:
Myth 1: “Every supplement needs a loading phase.” Most don’t. The vast majority of supplements — including magnesium, zinc, vitamin C, CoQ10, and probiotics — are taken at a consistent dose from day one. Loading phases are the exception, not the rule.
Myth 2: “More is always faster.” For fat-soluble vitamins, mega-dosing can backfire. Research shows that very large single bolus doses of vitamin D can paradoxically reduce effectiveness by triggering enzymes that break it down faster. Steady, moderate loading beats erratic mega-dosing.
Myth 3: “You can feel the loading phase working immediately.” With the exception of creatine (where performance effects may be noticeable within days), most loading phase effects are measurable only through blood work — not subjective feeling. Vitamin D levels rise gradually over weeks; iron stores rebuild over months. If someone is selling you a supplement with a “loading phase” and promising you’ll feel different in 48 hours, be skeptical.
Myth 4: “Omega-3s need a loading phase.” They don’t. Omega-3 fatty acids take 4–6 weeks to reach steady-state levels in cell membranes, but this happens at a consistent dose. The 2–4g/day prescribed for high triglycerides is a sustained therapeutic dose, not a loading dose that you later reduce.
Myth 5: “If a loading phase is good, a longer loading phase is better.” Loading phases have defined endpoints for a reason. Extending a vitamin D loading phase beyond the recommended 8–12 weeks without re-checking levels risks accumulation toward toxicity. Continuing high-dose iron after stores are replete causes iron overload. Always retest at the end of the loading period.
Risks and Side Effects to Watch For
Loading phases are generally safe when medically supervised — but “higher dose” always means “higher stakes.”
Common issues during loading:
- GI discomfort — Creatine loading can cause bloating, cramping, or diarrhea. Splitting the 20g into four 5g doses with meals helps. Iron loading commonly causes constipation, nausea, or dark stools — alternate-day dosing reduces these side effects significantly.
- Fat-soluble vitamin accumulation — Vitamins A, D, E, and K are stored in fat tissue and can build up to toxic levels. Vitamin D toxicity (hypercalcemia) is rare at standard loading doses but serious — symptoms include nausea, confusion, excessive thirst, frequent urination, and kidney damage.
- Iron overload — Excess iron causes oxidative damage to the liver, heart, and endocrine system. This is why iron loading requires monitoring ferritin and transferrin saturation levels every 3 months. Ferritin above 300 ng/mL or transferrin saturation above 45% is a signal to stop or reduce.
- Water retention — Creatine loading typically causes 2–4 lbs (1–2 kg) of water weight gain due to its osmotic effect in muscle cells. This is normal, harmless, and temporary — but it surprises people who aren’t expecting it.
Red flags to watch for during any loading phase:
- Persistent nausea or vomiting
- Unusual fatigue, confusion, or brain fog that worsens (not improves) during loading
- Dark urine or significant changes in urination frequency
- Severe GI distress that doesn’t improve after the first few days
- Heart palpitations or muscle twitching
If you experience any of these, contact your healthcare provider and consider pausing the loading dose until you’ve been evaluated.
Tracking Your Loading Phase
Here’s where loading phases get tricky in practice: your dose changes mid-protocol.
For six to twelve weeks, you’re taking one dose. Then you switch to a completely different dose — sometimes on a different schedule entirely (weekly to daily, for example). If you’re managing multiple supplements with different transition dates, it’s easy to lose track of when to step down.
Missed transitions are more common than you’d think. People finish their vitamin D loading course and keep taking 50,000 IU/week for months because they forgot to switch — or they drop the dose too early and their levels plateau short of the target.
This is exactly the kind of complexity that Gulpify is built to handle. You can set up a loading-to-maintenance schedule that automatically transitions your dose and reminders when the loading phase ends — no sticky notes, no calendar math, no forgotten step-down dates. Your tracking adapts with you.

Whether you’re tracking a single vitamin D loading protocol or juggling iron, B12, and D simultaneously — having your schedule in one place means one less thing to think about during recovery.
Key Takeaways
- A loading phase is a short period of higher-dose supplementation designed to rapidly bring depleted nutrient levels up to a therapeutic range before transitioning to a maintenance dose. Not to be confused with a build-up period where the dose stays the same.
- Loading phases have strong clinical evidence for vitamin D, creatine, iron, and B12. Most other supplements — including omega-3, magnesium, and zinc — don’t use true loading protocols.
- Blood work is essential before starting a loading phase. Don’t guess your levels — test them. The severity of your deficiency directly determines the loading protocol.
- The right loading dose depends on deficiency severity, body weight, absorption ability, nutrient half-life, and toxicity threshold. Vitamin D protocols differ significantly between someone at 8 ng/mL vs 18 ng/mL.
- Newer iron guidelines (ASH 2024) favor alternate-day dosing over daily loading for better absorption and fewer side effects.
- For anything beyond creatine, work with a healthcare provider to set the dose and monitor progress. Iron and B12 loading in particular require medical supervision.
- Watch for side effects — GI distress, water retention (creatine), or signs of toxicity (fat-soluble vitamins, iron) — and report them promptly.
- Don’t extend loading phases beyond the recommended duration without retesting. Recheck your blood work at the end of every loading period.
- Tracking matters because your dose and schedule change mid-protocol. Tools like Gulpify can automate the loading-to-maintenance transition so you don’t miss the step-down.
- When in doubt: test, don’t guess. Load with guidance, maintain with consistency.
Sources
- Holick MF et al. “Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline.” Journal of Clinical Endocrinology & Metabolism, 2011; 96(7):1911-1930. doi:10.1210/jc.2011-0385
- Kreider RB et al. “International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation.” Journal of the International Society of Sports Nutrition, 2017; 14:18. doi:10.1186/s12970-017-0173-z
- DeLoughery TG. “Iron Deficiency Anemia.” Medical Clinics of North America, 2017; 101(2):319-332. doi:10.1016/j.mcna.2016.09.004
- American Society of Hematology. “Iron-Deficiency Anemia Guidelines.” Blood Advances, 2020; 4(7):1501. Link
- Stabler SP. “Vitamin B12 Deficiency.” New England Journal of Medicine, 2013; 368:149-160. doi:10.1056/NEJMcp1113996
- NIH Office of Dietary Supplements. Fact sheets for vitamin D, iron, and B12. ods.od.nih.gov